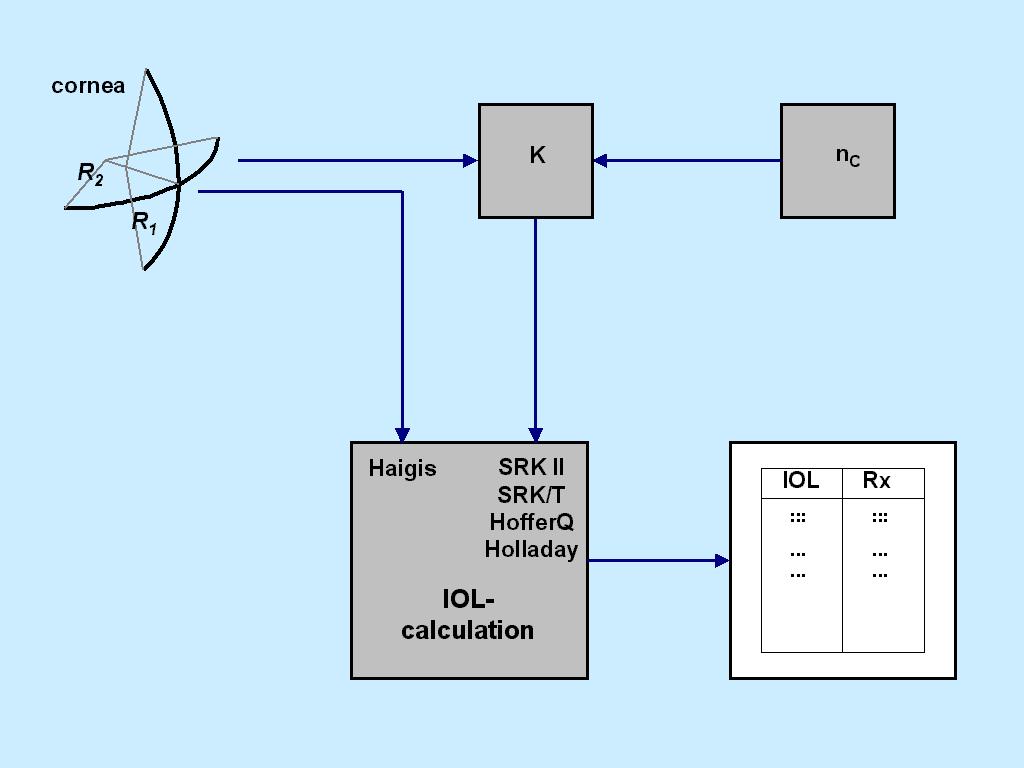
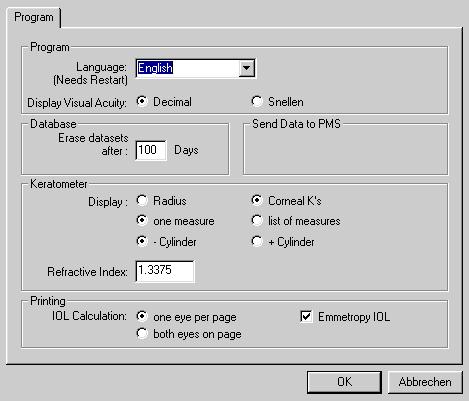
| Fig.2: If, in the IOLMaster, Ks are manually entered in diopters, the refractive
index set here (under 'options-setup-program-keratometer-refractive index') is used to convert
Ks into radii. Each IOL formula in the IOLMaster by itself makes sure internally that the correct conversion
is subsequently applied for power calculations. This setting, however, is only relevant if K readings are
manually entered in diopters. In case the IOLMaster keratometry is used for IOL calculation, no problems occur.
|

 ULIB Homepage
ULIB Homepage